
1. 위매독의 임상적 특징
Gastric syphilis의 특징을 정리하면 아래와 같습니다.
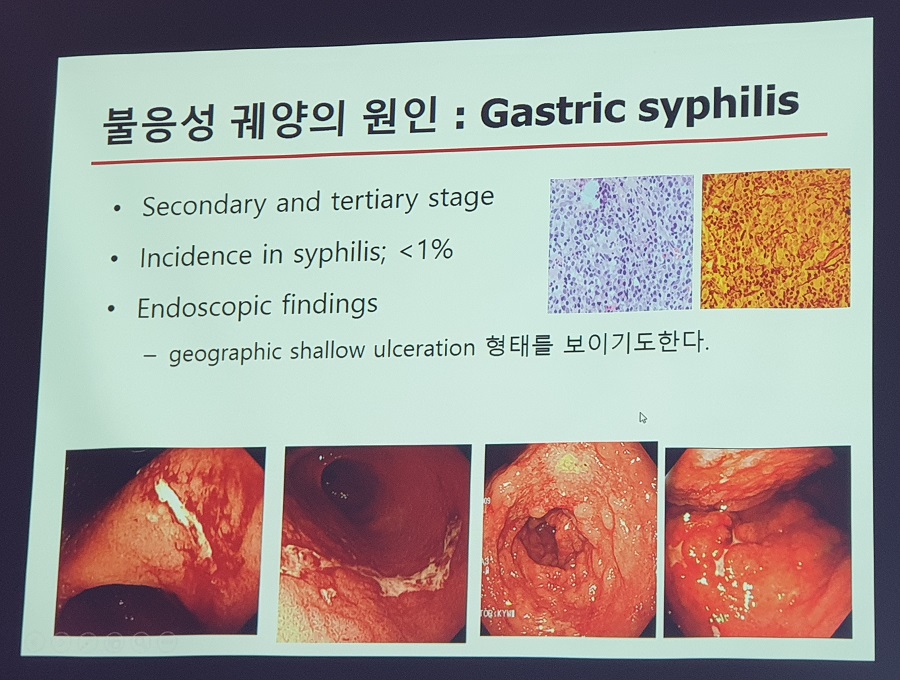
1. Secondary and tertiary stage
2. Incidence in syphilis; <1%
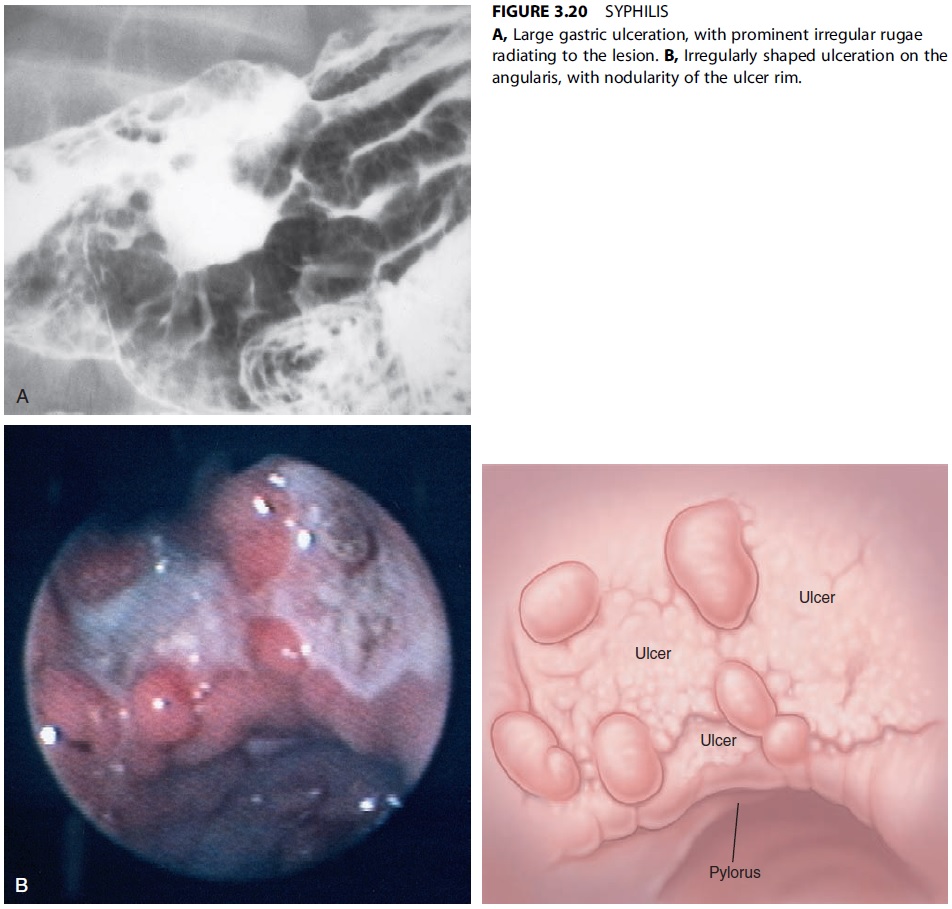
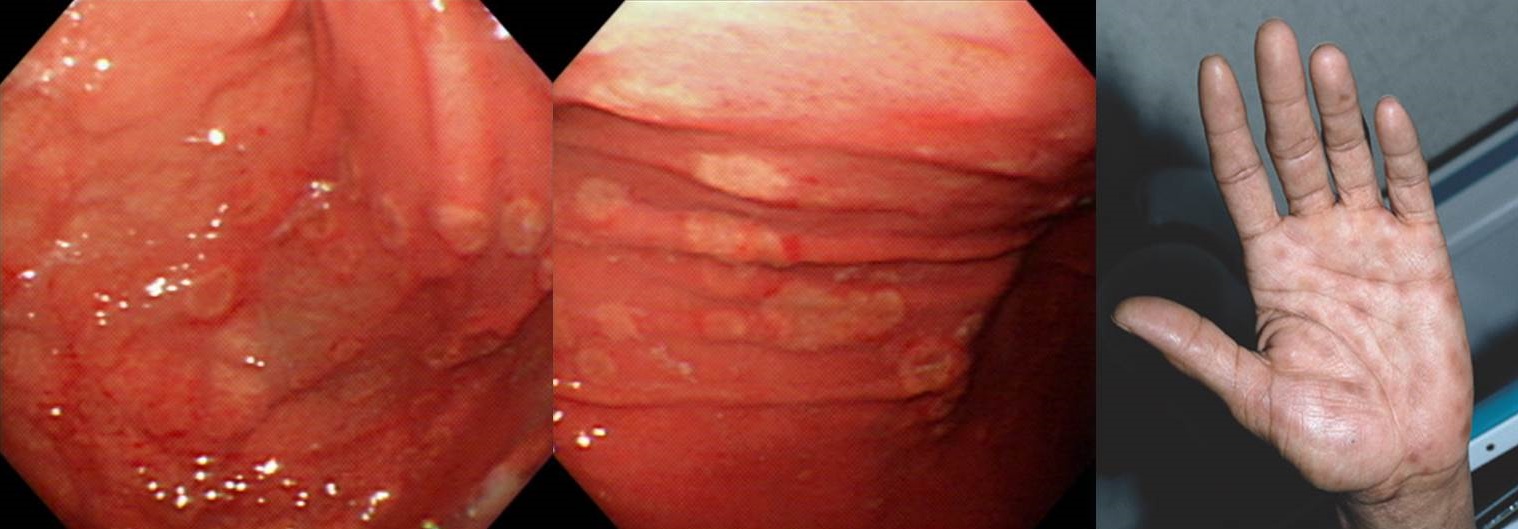
3. Endoscopy; erosive gastritis or gastric ulcer with heaped, nodular edges or thickened, edematous rugal folds.
4. Histopathologic findings; suggestive, but not diagnostic
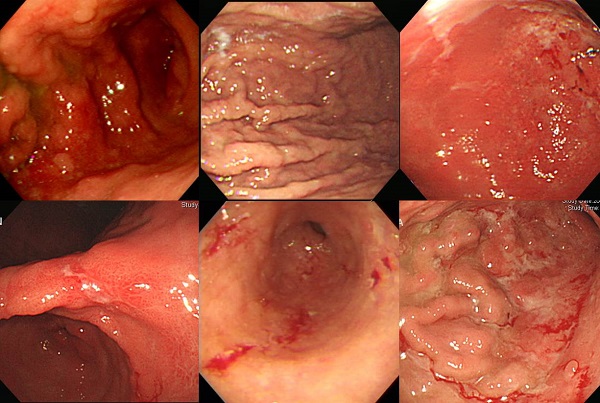
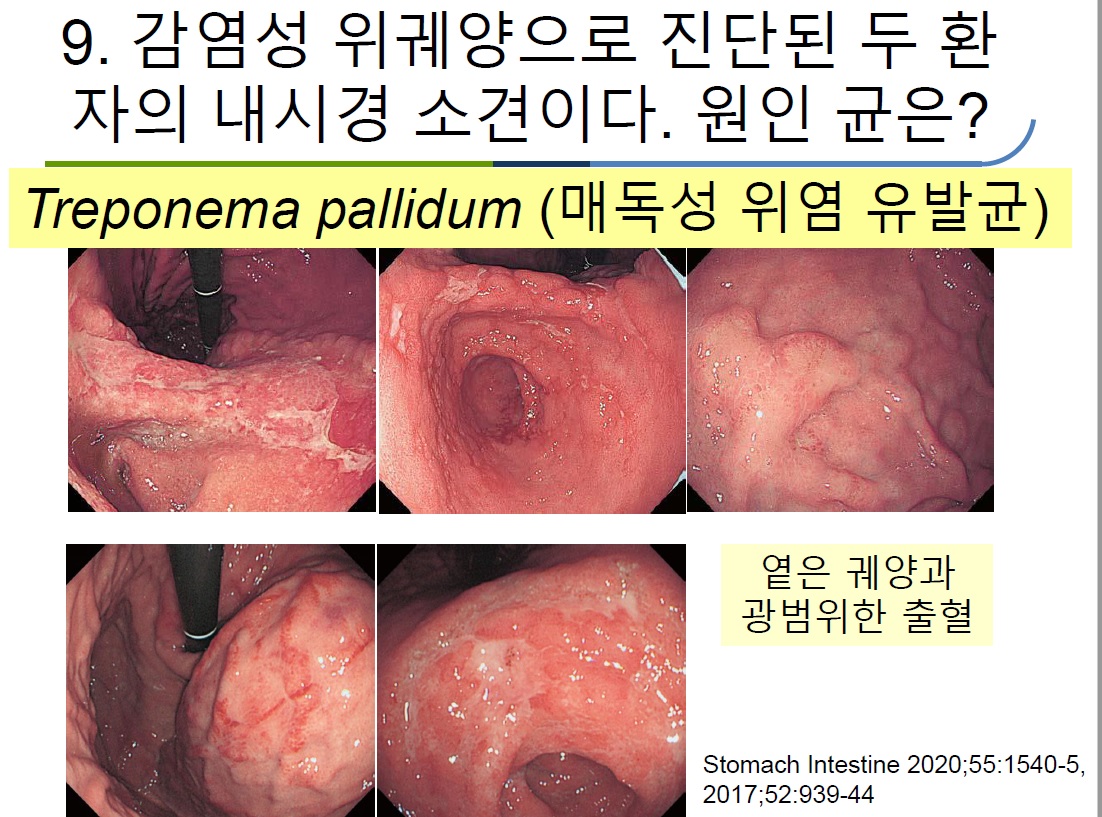
2. 위매독의 내시경 소견
제가 지금까지 알고 있는 gastric syphilis 6예의 사진입니다. 특히 첫번째 증례는 보만 4형 진행성 위암과 비슷하다고 의뢰되었던 경우입니다.
(2015)
2020-2-1. 부산경남지회 심포지엄. 좋은삼성병원 이태영
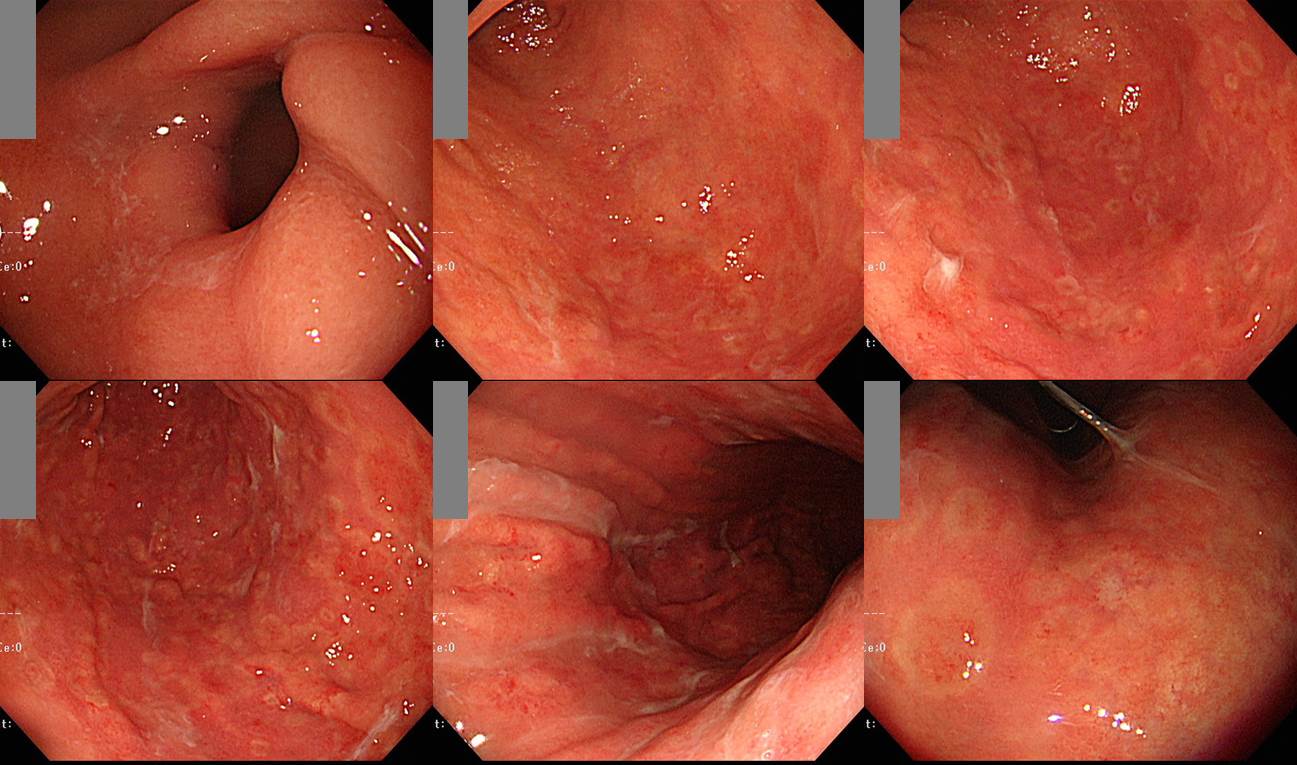

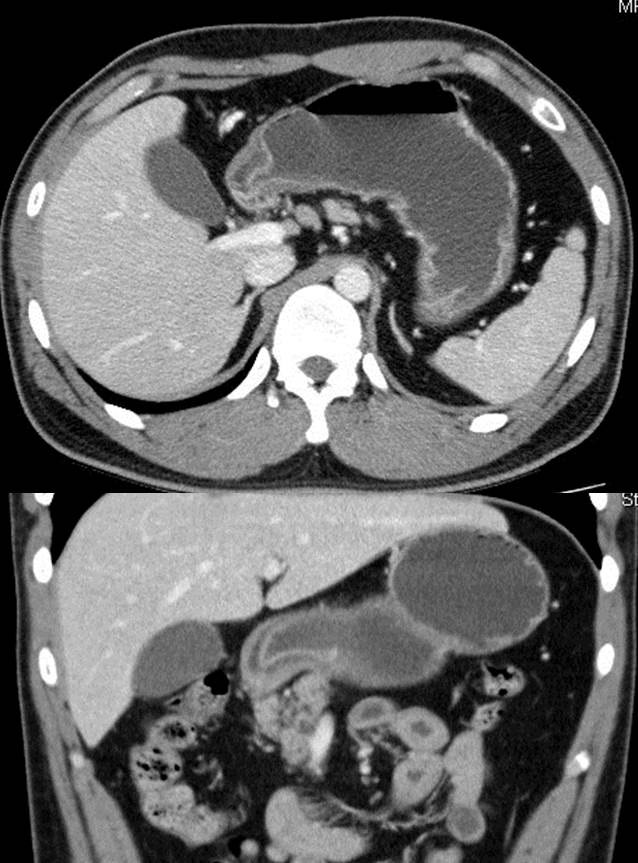
History: A 25-year-old, apparently healthy man presented with one month history of epigastric tenderness and vomiting. The patient visited a local clinic where he underwent an endoscopic examination and the endoscopic diagnosis was benign gastric ulcer. But gastric ulcer symptom was not improved on ulcer medication. He was transferred to our hospital for further evaluation. His family history and past medical history were negative for any gastrointestinal disease, abdominal surgery or significant medical illness. Physical examinations were normal except minimal epigastric tenderness only. A laboratory evaluation revealed hemoglobin of 16.4 g/dL and hematocrit 47.9%. White blood cell count and differential count were within normal ranges. Total serum protein level was 7.3 g/dL and albumin level 4.3 g/dL. Serum bilirubin and liver enzymes were within normal ranges. A computed tomographic scan of the abdomen with contrast revealed diffuse layered thickening of the wall of the gastric antrum, pylorus, duodenal bulb, and second portion of duodenal loop without definite perigastric and periduodenal fatty infiltration (Fig. 1). Multiple small and enlarged lymph nodes were identified along both common femoral vessel and inguinal area. Gastric endoscopy showed geographic irregular ulcer and shallow depressed mucosal lesions in almost all aspect of the antrum. The ulcer revealed an irregular edge and uneven nodular base (Fig. 2). Endoscope was failed to advance to the duodenal bulb due to luminal obstruction. A diagnostic procedure was done.
Biopsy: Chronic gastritis, active, with intestinal metaplasia (incomplete type), large lymphoid follicle and dense lymphoplasma cell infiltration ( Note: Based on histology, syphilitic gastritis could be considered)
Layered wall thickening involving gastric antrum, pylorus, duodenal bulb,and 2nd duodenal loop
Automated Quantitative RPR Test: Reactive(5.00)
Automated Quantitative TPLA Test: Reactive(282.9)
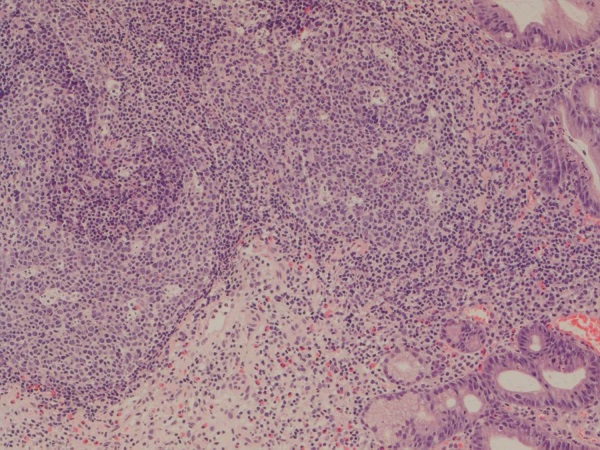
A: foveolar pit 에서 H.pylori 가 관찰되지 않는다. B: 심한 위염소견으로 neutrophilic infiltration 이 관찰된다. C: lamina propria 에 심한 lymphoplasma cell infiltration 이 관찰된다. D: lagre irregular lymphoid follicular hyperplasia with geographic feature
Large irregular lymphoid follicle : H.pylori 감염과는 달리 marginal zone 은 상대적으로 위축되어 있으나 follicular center 가 심하게 늘어나면서 지도모양(geographic feature) 으로 커져있다.

CPC에서 논의되었던 이 환자는 증례보고를 하였습니다 (위와 십이지장을 침범한 매독 1예).
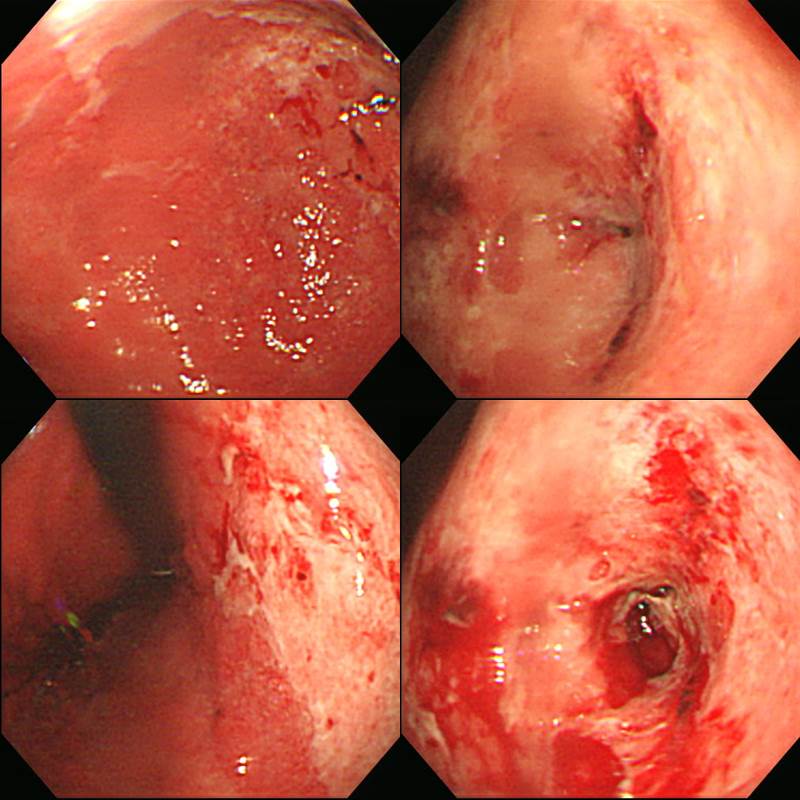
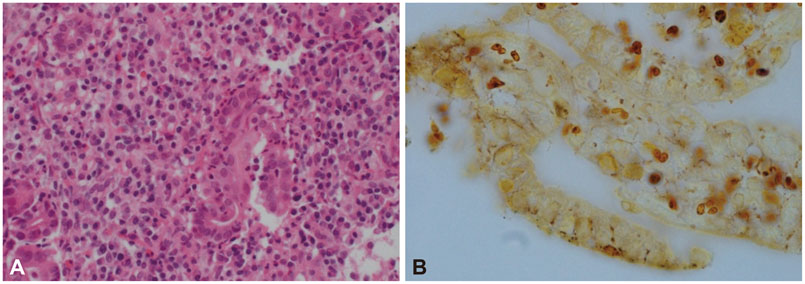
신증후군을 동반한 위매독 (Clin Endosc 2015). Gastroscopic findings. Multiple irregular, shallow ulcers covered with whitish exudates and central depression in the (A) antrum, (B) body, and (C) cardia. Histologic findings of gastric biopsy. (A) Marked severe inflammation with lymphoplasmacytic infiltrates (H&E stain, ×400). (B) Numerous spirochetes are present between foveolar epithelial cells (Warthin-Starry stain, ×1,000).
제82회 내시경학회 집담회 증례 (2008)
제82회 내시경학회 집담회 증례 (2008)
건국대 내시경 퀴즈 (2021)


댓글 없음:
댓글 쓰기