
위암 조직형과 분화도의 큰 줄기 - 우리나라에서는 대강 WHO 기준을 따르고 있습니다.
1998년 일본위암분류(1998)에서 일본 외과의사들이 이해하는 위암의 조직학적 분류는 아래 그림과 같습니다. "The histological classification should be based on the prominant pattern of tumor"라고 언급하고 있습니다. 여기서 "prominant"는 우리나라 병리 가이드라인(2005)에서 언급한 "암세포의 면적이 가장 많은 유형"과 비슷한 의미로 생각됩니다.

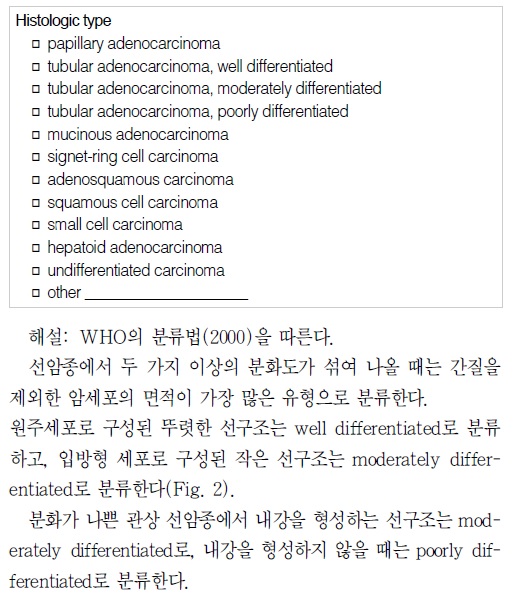
2005년 병리 가이드라인 (대한병리학회 소화기병리학연구회, 위암 병리보고서 기재사항 표준화, PDF 0.3M)은 (1) 위암의 histologic type은 2000년 WHO 분류를 따름, (2) 두 가지 이상의 분화도가 섞여 나올 때는 간질을 제외한 암세포의 면적이 가장 많은 유형으로 분류함, (3) 선구조나 편평상피 분화가 없는 경우에는 undifferentiated carcinoma로 분류한다고 명시했습니다.

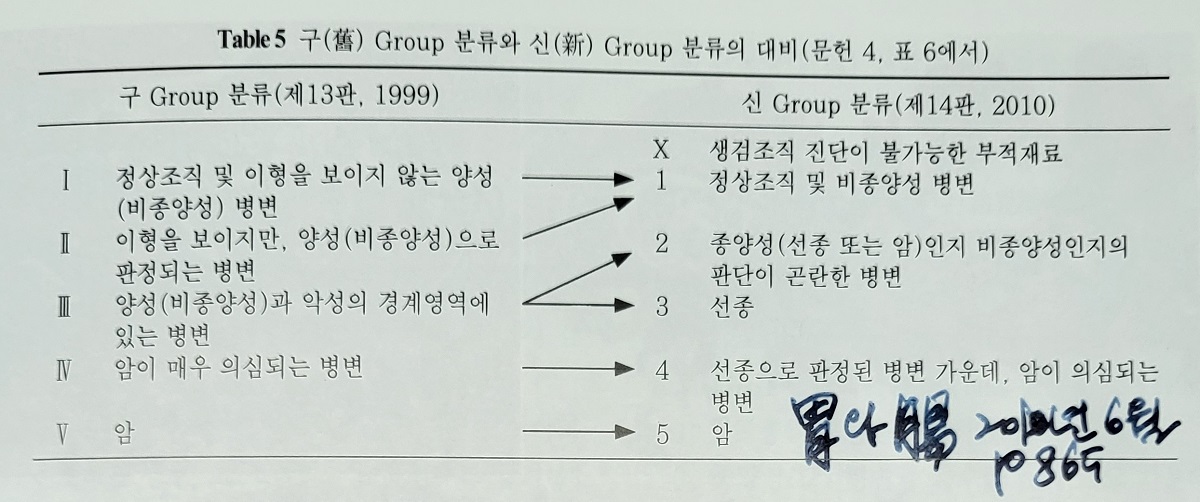
2010년 일본위암취급규약 제14판에 따르면 위암의 분화도는 선관형성 상태에 따라 고분화형, 중분화형, 저분화형으로 분류된다. 여기에는 세포형질의 분화 경향과 핵이형도는 고려되지 않는다 (위와장 2010년 6월호 857쪽). → [이준행 생각] Structural atypia에 따라 분화도를 나누고 cellular atypia는 고려되지 않는다는 의미인 것 같다. 그런데 보통 structural atypia는 cellular atypia와 함께 발생한다. 간혹 Cellular atypia는 거의 없는데 structural atypia만 보이는 경우 '저이형도 분화형 위암'이라고 부른다. 예를 들어 foveolar type, fundic gland type, intestinal type, crawling type (WHYX lesion)등이 여기에 해당한다.
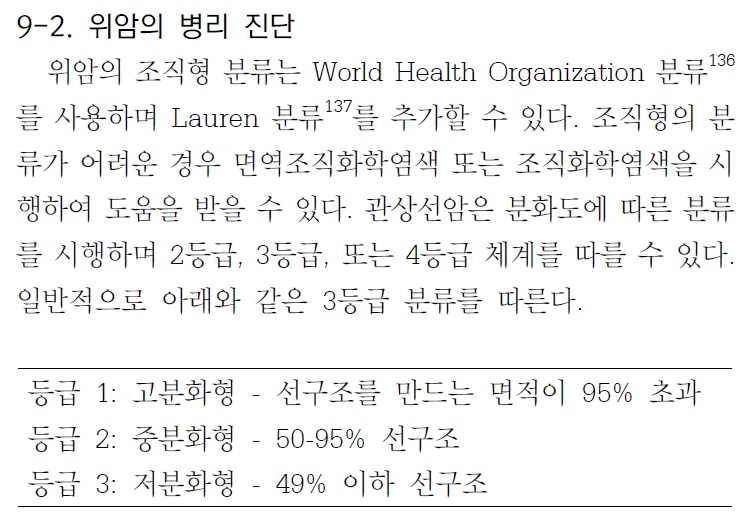
2014년 우리나라 다학제 위암진료권고안(제가 간사로 참여하였습니다)에서는 (1) 선구조를 만드는 면적이 95% 초과하면 고분화형, (2) 선구조를 만드는 면적이 50-95%면 중분화형, (3) 선구조를 만드는 면적이 49%이하면 저분화형으로 구체적인 수치를 언급하였습니다.

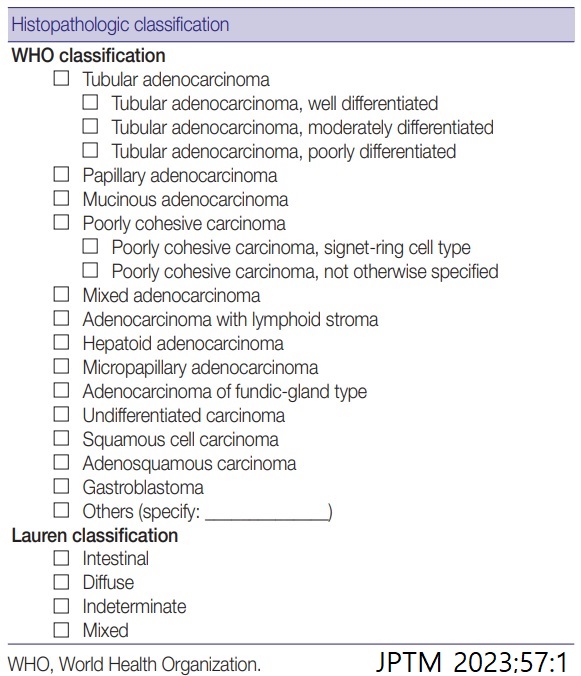
2023년 병리 가이드라인에서는 2019년 WHO classification을 거의 그대로 제시하였습니다.
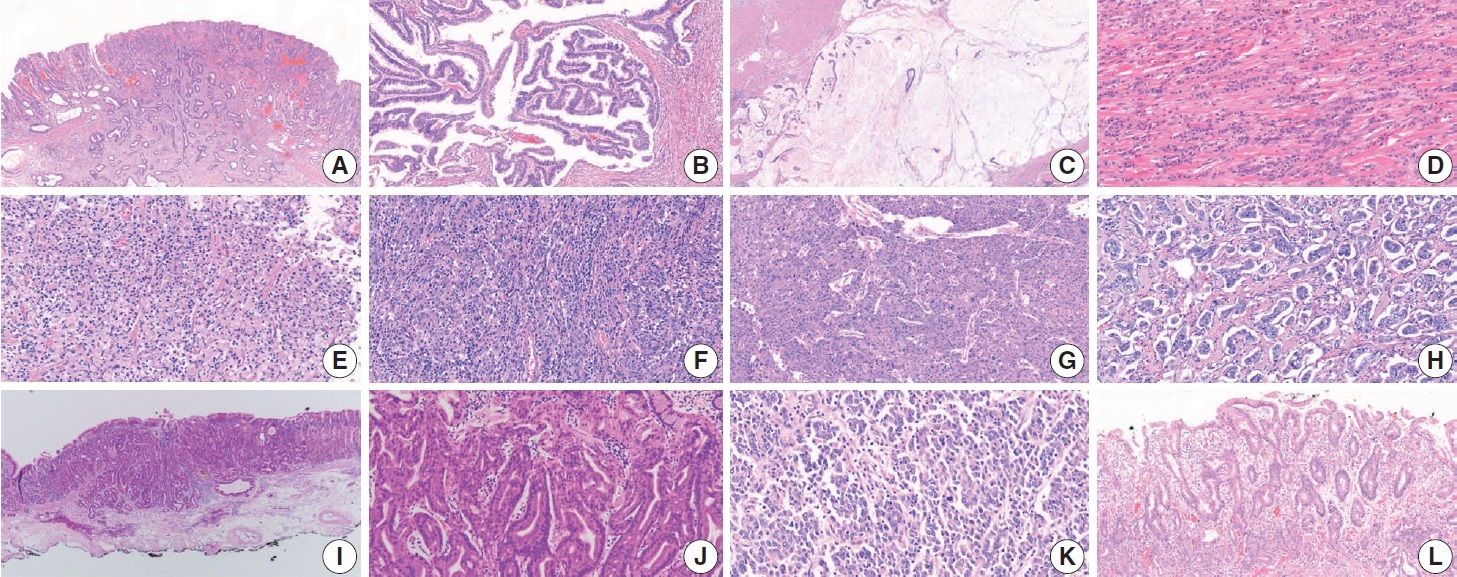
Fig. 7. Representative pictures of each histologic subtype of gastric carcinoma. Tubular adenocarcinoma (A), papillary adenocarcinoma (B), mucinous adenocarcinoma (C), poorly cohesive carcinoma, not otherwise specified (D), poorly cohesive carcinoma, signet-ring cell type (E), adenocarcinoma with lymphoid stroma 림프구버팀질동반샘암종 (F), hepatoid adenocarcinoma (G), micropapillary adenocarcinoma (H), adenocarcinoma of the fundic-gland type (I, J), undifferentiated carcinoma (K), and crawling-type adenocarcinoma (L).
2023년 병리 가이드라인의 tubular adenocarcinoma의 differentiation에 대해 아래와 같은 설명이 있습니다. 비전문가인 저는 다소 혼동스럽습니다. MD는 (1) cuboidal or flat cells 이거나 (2) distinct하지만 frequent luminal structures라는 것입니다. 면적뿐 아니라 세포형도 고려하는 것 같습니다.
"Tubular adenocarcinoma and papillary adenocarcinoma can be graded. When two or more differentiations are mixed in an adenocarcinoma, the differentiation grade reflects the largest tumor area. A distinct glandular structure composed of columnar cells is classified as WD, and a small glandular structure composed of cuboidal or flat cells is classified as MD. In a tumor with an in distinct glandular structure, carcinoma forming frequent luminal structures is classified as MD, and that with a rare luminal structure is classified as PD. Although the WHO recommends a two-tier grading system of low- (WD and MD) and high-grade (PD), most pathologists and clinicians use a three-tier grading system. We have agreed to used a three-tier grading system that can be easily switched to a two-tier grading system."
Grading of gastric tubular adenocarcinoma. Well-differentiated adenocarcinoma showing glandular structures composed of columnar tumor cells (A). Moderately differentiated adenocarcinoma exhibits more complex tubular structures with cuboidal and/or flat epithelial cells (B). Tubular structure is unclear in most tumor glands in poorly differentiated adenocarcinoma (C).

[2023년 종설] 샘암종의 분화도는 주로 관샘암종과 유두모양샘암종에 적용된다. 뚜렷한 샘 구조를 만드는 종양으로 주로 원주형 세포로 구성된 경우 고분화(well differentiated)로, 샘구조가 뚜렷하지만 샘들의 크기가 작고 입방형이나 납작한 세포가 주 구성세포인 경우 중등도 분화(moderately differentiated)로 분류되고, 내강 구조를 거의 형성하지 않을 때는 저분화(poorly differentiated)로 분류된다.20 한 종양 내에서 두 가지 혹은 그 이상의 분화가 혼합되어 관찰될 경우, 일반적으로 가장 많은 부위에서 관찰되는 분화도에 따라 등급을 결정한다. (위암 병리 소견의 이해 김백희, 이성학. 헬리코박터학회지 종설, 2023)
댓글 없음:
댓글 쓰기